
Part One of this series discussed the epidemiological evidence that masks don’t curb spread. Part Two talked about the dynamics of droplets versus aerosols. (Incidentally, this study was just published finding 85% of the virus spread was found in fine aerosols.) Now let’s get into viral interference, to put to rest the idea that masks stopped the flu this last year.
When the mask mandates first came out, I suspected they wouldn’t last for very long. I had two thoughts. First, I figured that the second that people realized that they were still getting colds, flus, and other respiratory bugs, their logic muscles would kick in. They would realize that if the mask didn’t stop them from catching a cold, then it wouldn’t stop them from catching COVID. (I also misunderstood how masks would become tribal badge and religious totem.)
Second, I suspected that winter 2020 would be unprecedentedly awful, as COVID and the flu simultaneously ravaged through the community and we had a double hit of respiratory disease.
I was wrong about both, but for the same surprising reason.
Part III: Viral interference needs better public relations
This is where my unified-field-theory approach works pretty well. We need an explanation for why masks don’t work for COVID, but why flu apparently disappeared starting spring 2020.
What if masks don’t work for COVID, but do work for the flu? Maybe the particle sizes are different or behave differently?
We can answer this question by looking at countries that didn’t have mask mandates, or at least had low mask adherence. Maybe a comparison between Sweden, Australia, and the US?
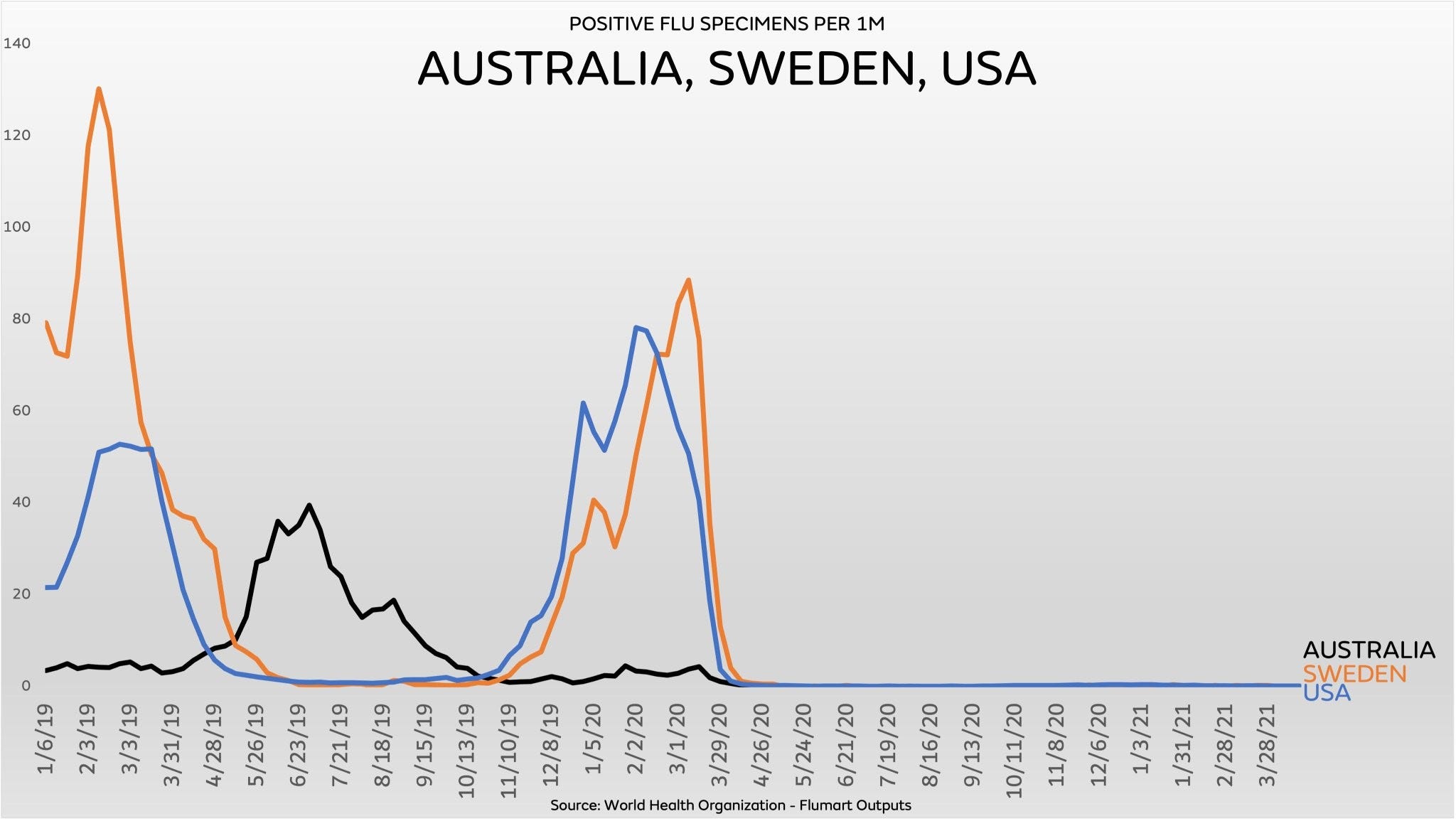
Huh. The flu disappeared there too, despite Sweden never passing a mask mandate and, last time I checked, having 9% mask compliance.
And thanks to the site syndromictrends.com, which charts the prevalence of different viruses over time, parainfluenza and respiratory syncytial virus (the two purple blobs at the top), were gone until they started to grow again in March, outside of their usual winter seasonality.. Influenzas A and B left the virome in April 2020 and still haven’t come back.

There was an idea that caught fire in the last week or two, as the FDA changed its authorization for the PCR test. A poor interpretation led many on Twitter to believe that the PCR test couldn’t differentiate COVID and influenza, due to the COVID PCR using the flu virus to calibrate. This article puts that idea to rest. The PCR test we’ve been using since spring 2020 clearly can tell COVID from influenza.
So let me introduce you to the concept of “viral competition”. When there’s a big new bug in an area, it bullies every other similar bug into the background due to its infectivity. If you’re susceptible to a respiratory virus at that time, you’re just going to get the Big New Virus until that’s infected enough people that it takes its place among the rest of the gang. These “endemic” viruses then just come and go with the seasons, as Edgar Hope-Simpson observed in the 1980s.

This is important, because there’s a defined, observable seasonality to viruses, which come and go based on the outside weather, how people are congregating, indoor air conditions, etc. This is why the Sun Belt is having a Delta wave presently — not because it’s a worse, scarier COVID, but because everyone’s spending time inside in the southern areas of the US, and here in Missouri where we just had a miserable heat wave.
This video by Ivor Cummins has a very good and succinct explanation.
Back to viral interference. Check out this piece in Stat. It observes that during the H1N1 outbreaks in 2009, France braced for it to hit their shores. But it didn’t, only infecting their population months later. It’s theorized that a particularly nasty rhinovirus was working its way through the French population, infecting all that it could and muscling H1N1 out of the way until it had reached its natural peak.
To be fair, there probably is an effect of the increase in working-from-home and the decrease of people in public spaces that could be causing a decrease in respiratory disease infection as well. It’s not a stretch to think that increased diligence in washing hands and an increase in people working out of their basements (like me!) could have an effect.
But the question then becomes “at what cost long-term”. The evidence as I understand it says that the human immune system needs to be trained, encouraged, built up. If you go to live in a bubble for five years, when you come out you’re going to be susceptible to any number of things you would’ve been able to fight off without a problem before.
I believe this - viral competition and untrained immune systems - is why we’re now seeing record numbers of RSV cases. As COVID recedes, all of the viruses that have been competed into the background are allowed to come back. And the immune systems of people who have been around fewer other people now have to contend with it all over again. In fact, Tracy Høeg, MD theorized that the current increase in hospitalized children, which is being assigned to COVID, is actually RSV.
If new parents - of which I’m about to be - are keeping their babies home and safe, avoiding taking them out into the world where they can be exposed to all of society’s different dirts and grimes, then it makes sense that they’re more susceptible to something like RSV that, ironically, has a much higher mortality rate in their age range that does COVID.
This is the greater lesson of the last several months for me, and a more widely applicable one. One of the great unspoken stories of our time is the increase in narcissism. It’s inevitable with the rise of social media, as we all have new mirrors and ways to show off — and regular feedback in the form of likes, thumbs, and Instagram double-taps — we become more enamored with the idea that the world revolves around us, that other people are characters in the movie that is our lives.
This extends to public policy in a particularly devious way: my preferred policy will achieve my desired goal, and nothing else. Unintended consequences are ignored, dismissed, or outright denied. It’s not possible that masks, social distancing, stay-at-home policies could have serious negative consequences, because the experts have said that this is more important.
Like my previous newsletter about the failure to update priors, it’s the lack of imagination that bothers me. The failure to think outside the box and consider downstream effects is, frankly, baffling, and this is where I feel most helpless.
When the head of the Metropolitan St. Louis Hospital COVID Task Force gives a presentation and says that they are recommending keeping the mask mandate because models have told them what the results are, they’re presuming something that’s not in evidence. When Australia locks their population down for the sixth time, now enforced by the military, I wonder what they’re expecting that didn’t work in times one through five. And they are causing absolute misery for their residents in the meantime.

In the next newsletter, I’ll bring in some of the other things I’ve been thinking about and try to tie some of these thoughts together.