
I’m about to touch the third rail of COVID policy, the unquestionable idea that masks are effective. As the CDC has just last week updated their recommendation that vaccinated people should wear masks indoors again and mask mandates have been brought back (among some controversy) in my home St. Louis County, I had intended to launch this series this week and now the timing is perfect.
I hope my reputation as a calm, rational, and considered person precedes me here. My job as a data analyst is to consider the information I see, construct a narrative around it, and then consider any counterarguments that could undermine that narrative. I’ve considered these facts and all of the evidence that I could find, to the point where it’s kept me up at night. I hope that all of this consideration comes together to provide a point of view you may not have heard before, but will make instinctive sense to you as you consider what you see in the world.
Part One focuses on the scientific studies that about mask effectiveness and the population-wide evidence. Part Two will discuss the differences between droplets and aerosols and non-pharmaceutical interventions for each. Part Three will get into viral competition and why the flu disappeared in late winter 2020. And Part Four will consider things from a evolutionary or historical perspective, and hopefully explain why all of this matters.
Let’s get stuck in.
From April 2020 onward, people seemed to think that masks were going to be our temporary savior until the vaccines arrived. CDC Director Robert Redfield said in Congressional testimony that masks were actually more effective than vaccines. Every medical authority immediately got in line, publishing their recommendation for masks of any type - cloth, N95, medical, whatever you can get.
My initial thought was that they’re unlikely to do much, but I’m not the kind of person to make much of a stink about something that seems harmless at best. I dutifully wore my N95 while out shopping until the rubber bands broke, then started to wear cloth masks like most people.
If I had a thought against them, it was the possibility that if they didn’t work, they could be giving us false confidence and letting us get close to people without thought to social distancing, which might be the one thing that did work. At the least, it seemed like something that gave people confidence to leave their houses, which they might be disinclined to do otherwise.
Oh, I was so very wrong. But like any story worth telling, it’s incredibly complicated.
Part I: Science is probably broken
One of the things I learned about while doing my nutrition science deep dive was the perils of epidemiological science. Any time you see a headline stating “RED MEAT WILL INCREASE YOUR RISK OF HEART ATTACK BY 25%”, it’s based on an epidemiological study. The study creators polled several thousand people about what they ate, then followed them for several years and recorded what happened to who. It’s useful for generating hypotheses, which can then be tested with randomized controlled trials to control every variable and drill down on the actual effect.
That’s not what these studies are being used for. The studies actually say something like “the 4000 people who said they ate red meat more than four days a week had 8 heart attacks (8 / 4000 = .002), and the 5000 people who said they ate red meat once a week or less had 6 heart attacks (6 / 5000 = .0012), so there was a 60% greater incidence in the high-red-meat group”.
Let me introduce you to the most important concept you’ll learn today:
CORRELATION DOES NOT IMPLY CAUSATION.
In the above example, we aren’t told whether the people who ate more red meat also smoked more or ate fried foods more. We aren’t told whether the people who ate less red meat were runners, or ate salads four days a week. Therefore, we don’t know why they had more heart attacks unless the signal is SO strong that it can’t be ignored - in the thousands of percentage points (as was found in the epidemiological studies around cigarettes and lung cancer).
Knowing this caused me to look askance at every scientific study that made the news, because so often they were prone to problems like those above. This study in PLOS One correlated mask adherence with case rates, but who knows what could be affecting those case rates across different states, with different policies, with different populations, with different population health, with different geographical latitudes. This study from the NIH formed a barrier with mask fabric and sealed the tube around the edges to test permeability, which ignores the air leaks around the edges of the mask which greatly diminishes their efficiency. But these studies were touted by the media as proof that masks work against COVID.
Because of groupthink, it went unquestioned. Once the general consensus was that masks always work, any evidence to the contrary was ignored, shut out, or flat out silenced.
(To be fair, one could say this seems to be more of a problem with the way that science is reported, rather than science itself. From what I can see, science reporters are not taught to look for the flaws in studies, but dutifully repeat whatever is in the press release. But the peer review process should also catch these issues.)
Now let me introduce you to the converse of the previous logical concept:
THE LACK OF CORRELATION IMPLIES THE LACK OF CAUSATION.
Think of it this way. If A happens and then B happens, we don’t know if A caused B. But if A happens and B doesn’t happen, then we know that A cannot cause B.
What does this mean for masks? One of my favorite Substack writers is IM, who writes Unmasked. For the last several months, he’s been posting graphs on his Twitter account showing the lack of correlation between mask policies and case rates. Over and over again, countries, states, or counties that implemented mask mandates found no effect on how case counts went up or down.
For instance, Germany has had a fine-enforced mask mandate since April 2020, a surgical mask mandate since January 2021, the German state of Bavaria has had an N95 mandate since January 2021, and the city of Berlin has had an N95 mandate and a testing requirement since March 2021. Has the enforcement of high-quality masks helped?

Japan has been renowned for being a mask culture for decades, and has had mask compliance of more than 95% throughout the pandemic. Has that been effective?

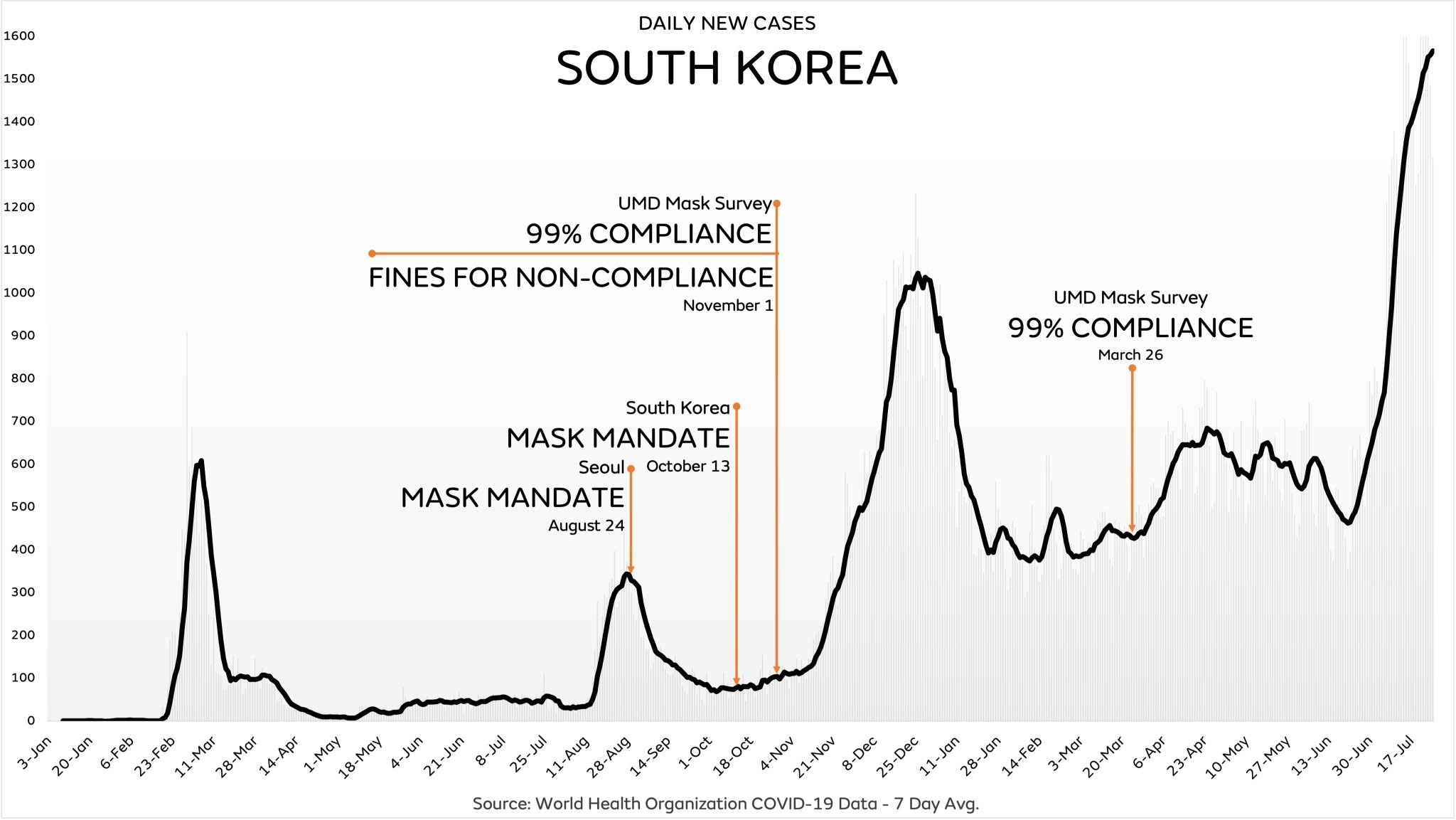
Nearby South Korea was initially praised for their response to the pandemic, have had a nationwide mask mandate since October 2020, and have had 99% compliance. How are they doing now?
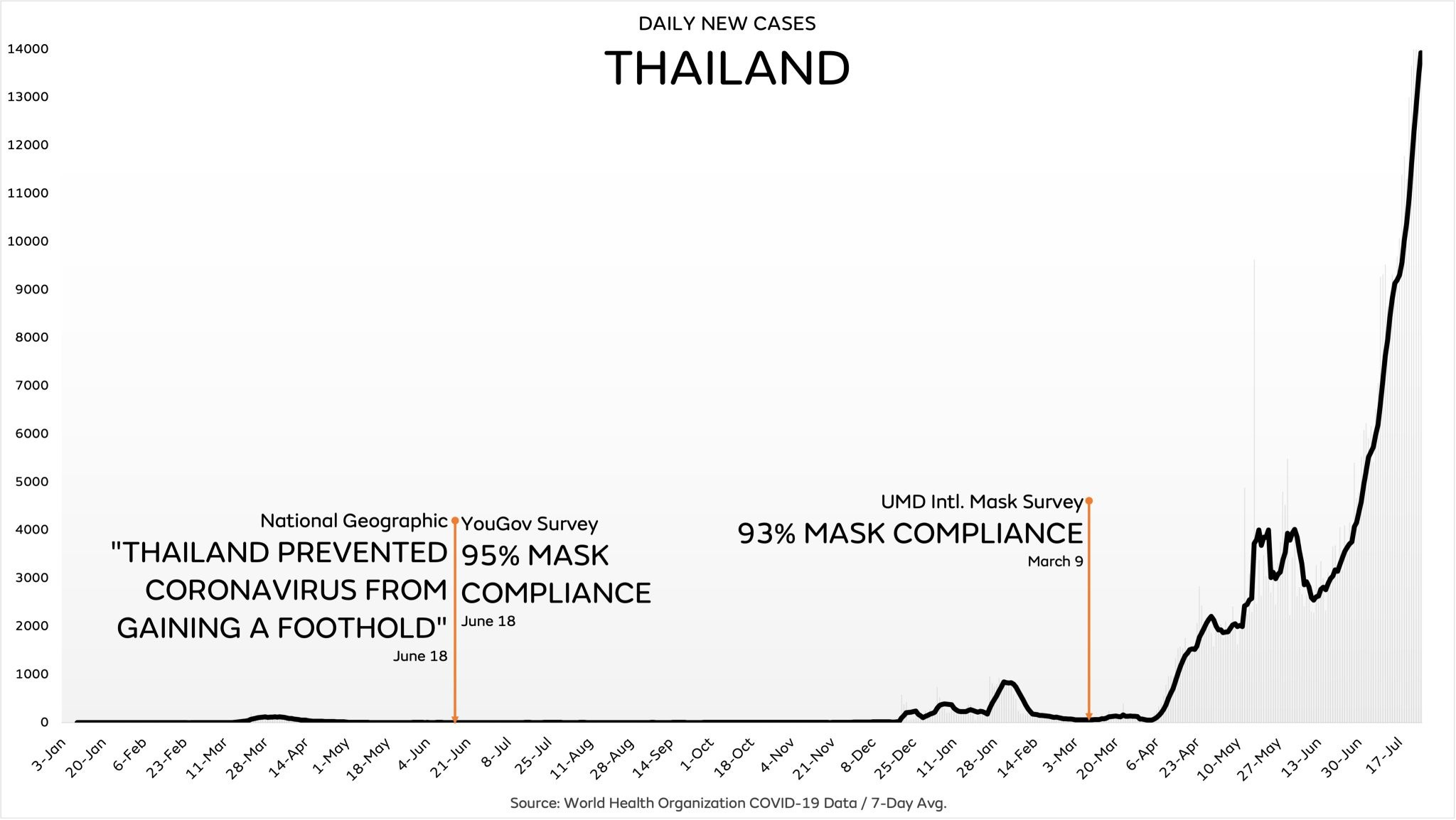
Thailand was praised in summer 2020 and has 90%+ mask compliance. How are they now?
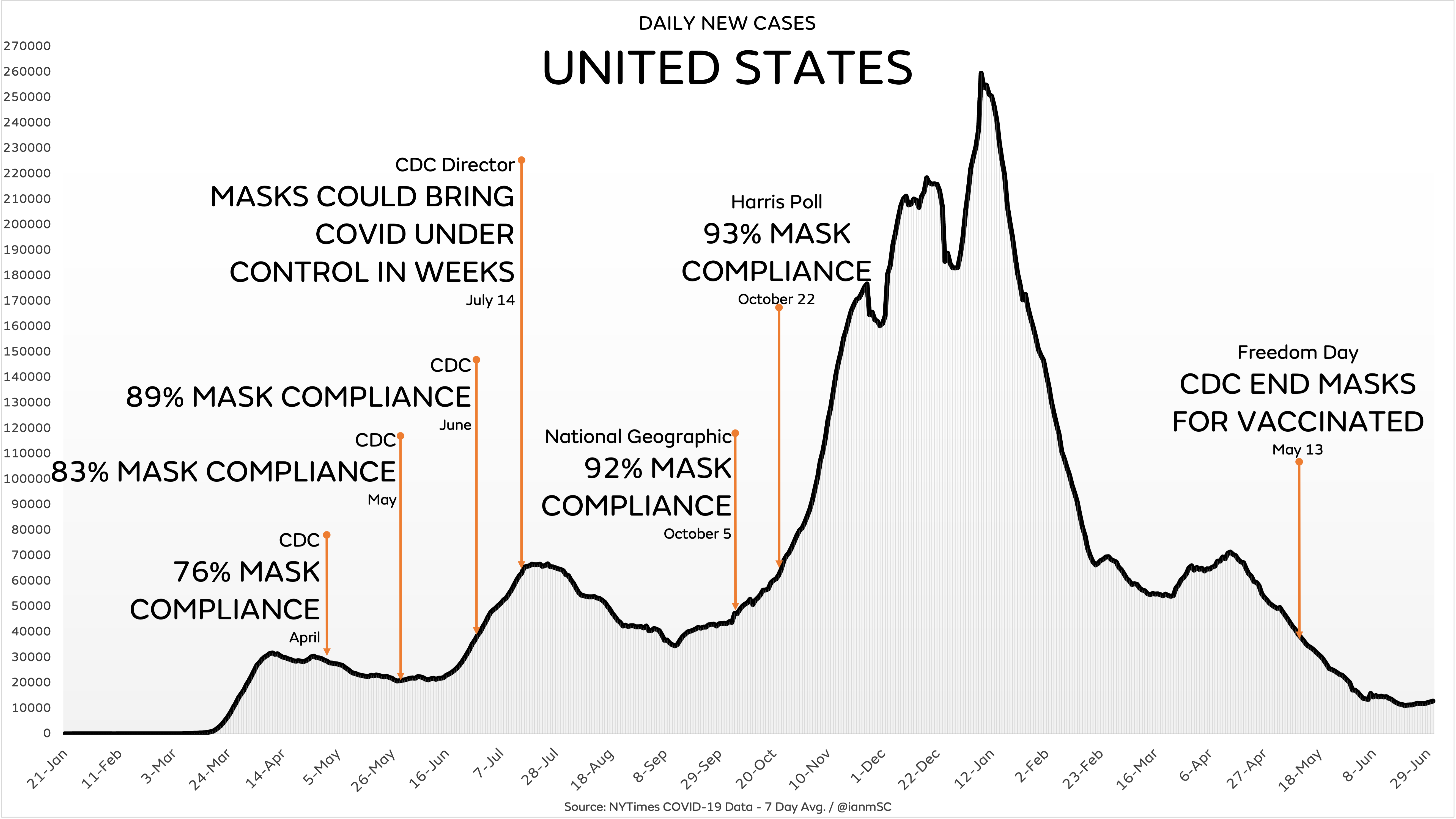
Here in our country, the director of the CDC said that masks could bring the pandemic under control within weeks. How did that work out?
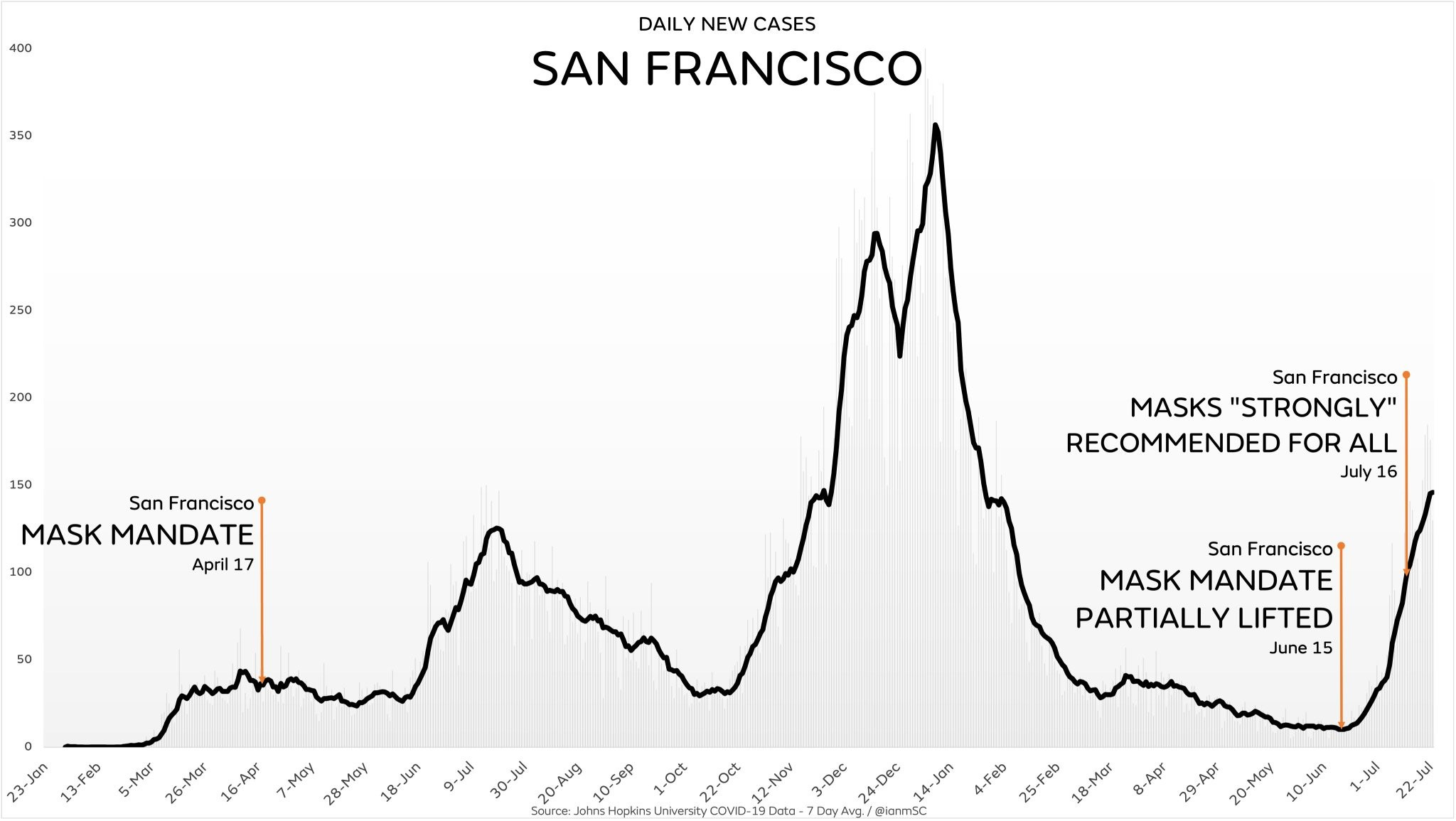
But this is clouded by a huge variety of policies, varying from state-to-state, county-to-county, and city-to-city. So let’s focus on one city, San Francisco, which had a mask mandate since April 2020. Did that save them?
I don’t know how someone can look at the graphs above and conclude that mask mandates work. Regardless of country or population, the case counts inevitably climb and recede of their own volition.
So several months ago, as I started to see case counts go up and down around the nation and the world regardless of mask mandates, my compromise position was that maybe masks work when worn perfectly, but there’s no evidence that mandates work because they can’t mandate that people wear masks correctly or that masks are well-constructed.
But as I considered more and did more research, I found how little masks do against respiratory viruses.
And that’s the subject of my next newsletter.