
Part One of this series discussed the scientific and epidemiological evidence for and against masks. Even the CDC should have reconsidered the evidence when they released their own study in which 71% of the positive cases reporting “always using cloth mask face coverings or other mask types when in public”. Let’s look at why masks are destined to fail against a respiratory virus such as SARS-CoV-2.
Part II: Droplets and aerosols have very different remediations
Think back to March and April 2020. We knew COVID was here, but we didn’t know much about it and we didn’t know how scary it actually was. We saw videos from China and Italy of packed hospital beds and apartments being welded shut. So, we took a maximal approach and hunkered down.
It looked at the time like the virus spread by droplets, so we took steps accordingly. We erected Plexiglass shields to minimize the range of coughs or sneezes. We told everyone to stand at least six feet apart. We started cleaning everything in sight, including our groceries and our mail. And, we started wearing masks to catch our droplets. Images like this one went viral:

Then at some point, we learned that COVID is not spread primarily by droplets, but by aerosols, which are smaller by orders of magnitude. The CDC’s transmission fact page currently acknowledges both droplets and aerosols, and this article from The Lancet makes the argument for aerosol transmission.
This matters because things that you can do to prevent droplets are useless against aerosols, and in some cases make the situation worse.
Think about the Plexiglass shields. If it’s there as a sneeze guard, it’ll do the job. But if the air that someone breathes out has virus particles itself, not carried by larger droplets, then their air will mix with the room air and circulate wherever it wants to go, like pouring cream in your coffee.
On top of that, this article from Bloomberg makes the argument that Plexiglass barriers such as these prevent the air from circulating properly. So a commercial HVAC system isn’t able to turn over the air in the same way because these pockets of stale air are formed by the barriers, so virus-laden air can’t be carried away and scrubbed.
So, why can’t a mask work against aerosols? Because most of the air exhaled by a person wearing a mask goes out the sides and up past the nose. Some is filtered by the cloth, but this is pretty ineffective. The size of aerosol particles that carry virus are less than 60 microns (a micron is one-millionth of a meter), while medical-grade masks have holes or at least 80 microns, and cloth masks can have holes of 500 microns. Even an N95, which theoretically can filter down to .3 microns, work much better at filtering when you’re breathing in than when you’re breathing out, because of the pressure building behind the mask. (And we know from the previously-cited data from Germany than N95 mandates don’t seem to be doing much either.)
This is a great explanation of the science of mask particle size by a viral immunologist.
Remember what I said in my last mask piece about science being broken? This study I just encountered tests mask efficiency for filtering out particles. Check out this image:
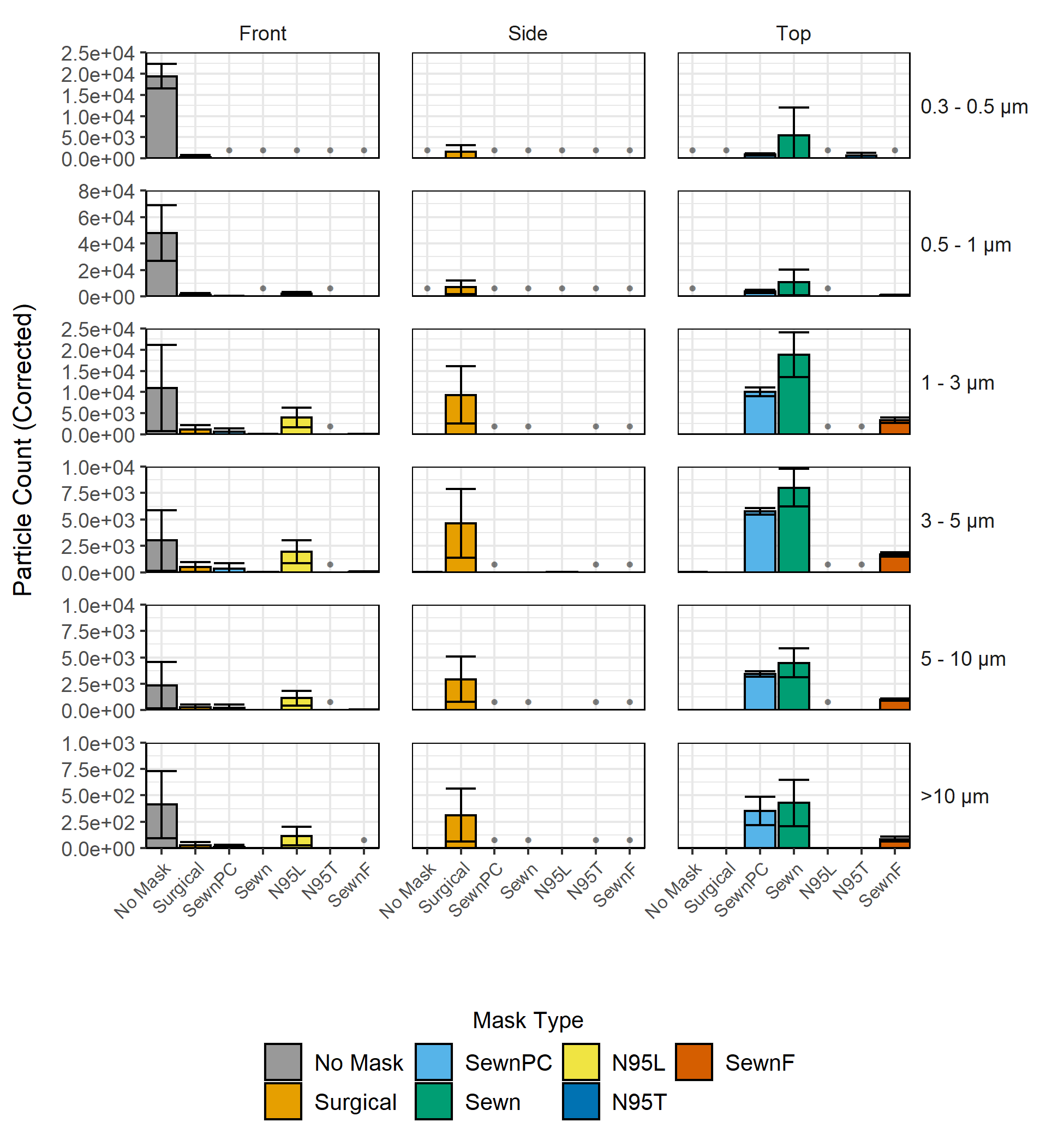
Remember, an aerosol particle is less than 60 microns. So we only need to worry about the bottom row, where there’s not much of a difference between wearing no mask at all, a surgical mask, a two-layer sewn mask, or a two-layer sewn mask with a pipe cleaner to create a tighter fit around the nose. In the surgical mask, it all just escaped around the sides, and in the cloth masks, it escaped around the nose. And this was in a lab study with a 3D printed head, not in a real-world test scenario.
There’s another level to this as well. As your mask is worn and the holes fill up with the moisture in your breath, those holes will fill up, and even more air will go out the edges. Worse than that, a PPE physics expert named Megan Mansell makes the case that as you exhale through your mask, the force of the air will aerosolize the larger particles, making you more infectious, not less.
The science of virus aerosol spread and masks has been known for years, because influenza spreads in a very similar way. This study published at the CDC analyzed ten studies on mask effectiveness for influenza, and while it acknowledges that most studies were underpowered, none of the ten studies showed a significant effect by mask wearing.
So one of my great frustrations as our COVID response goes on and on is that it appears to me that our public health officials and those in power aren’t updating their priors. Every time I see a cashier boxed in behind Plexiglass, or a person walking around with two masks, I wonder why public health officials haven’t come out as new information has come in and said something like, “We recommended things based on what we knew at the time, we now know something different, so let’s concentrate our efforts where they make a difference and let the other stuff go.”
Instead, officials are doubling down on what we now know doesn’t do anything. Cities and school districts are reinstating mask mandates, after months of real-world evidence that they don’t do a single thing to curb spread. Dr. Rochelle Walensky now says that every person - vaccinated, unvaccinated, old, young - in a K-12 school should wear a mask.


And the director of the NIH recommends wearing a mask inside your own house around your unvaccinated children.


Things have gotten weird.
“But Joshua,” I hear you saying, “the flu disappeared last year, and I haven’t gotten a cold since all this started. Surely the masks are responsible!”
I can answer that, and it’s a way more interesting answer than you think. But I’ll save it for my next newsletter.